 Tool -
Tool -
Behaviour Change Communication (BCC) refers to the strategic use of communications to positively influence people’s knowledge, attitudes, and practices. In the water sector, BCC has been heavily applied in the Water, Sanitation, and Hygiene (WASH) space (Dreibelbis et al., 2013), and to a lesser extent in irrigation (Blackstock et al., 2010) and disaster risk management (Bubeck et al., 2012). The approach uses a critical discernment of people’s behaviour and then aligns it with persuasive communication methodologies. Effective BCC requires, on the one hand, a strong knowledge of how individuals and communities think and act and, on the other, the customisation of messages and communication activities based on those observed needs and local realities. The tailored messages are then disseminated through various selected channels of communication, such as peer-to-peer, group, and mass media to bring about positive changes in behaviour regarding specific challenges. Behaviour change does not happen overnight, it requires sustained efforts by multiple stakeholders working at different levels.
Before getting into how to design a BCC strategy, we must first understand how behaviour change works at the individual level. The Transtheoretical Model of Health Behaviour Change suggests that there are six stages of changing ones behaviour (Prochaska and Velicer, 1997) (Figure 1):
- Pre-Contemplation: At this stage the individual is yet to determine a problem even exists in their behaviour.
- Contemplation: Acknowledgment of the problem begins, but the individual may not be ready to make a change.
- Preparation/Determination: Getting ready to make a change.
- Action/Willpower: Making decisive action towards changing behaviour. At this point the individual is undergoing increased awareness, education, and capacity building.
- Maintenance: Here the individual tries to consistently maintain the changed behaviour. In this regard, consistency can be linked to a cycle of information and engagement to create an environment that is conducive towards positive change.
- Termination: Full change occurs at this stage, the induvial does not return to old behaviour. Monitoring and evaluation is critical once this stage is reached to determine how effective was the change. “Slippage” or “relapse” may happen as certain individuals may return to old behaviours, especially if a conducive environment for change is not maintained.
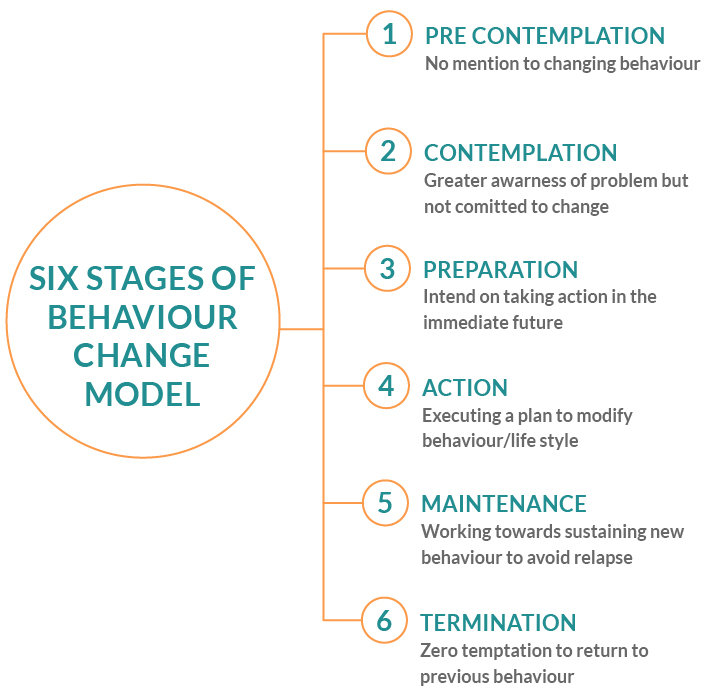
Figure 1. Transtheoretical Model Stages of Behaviour Change (Adapted from Prochaska and Diclemente,1997)
Here are the 6 steps for developing an impactful BCC programme strategy:
1. Enabler and Barrier Assessment: The first step to a successful BCC programme strategy is to carry out research about the target audience, including an extensive assessment of the behaviour to be changed and the reasons underpinning it. This requires assessing their knowledge, attitudes, needs, and habits (where do they seek information? On what platforms are they engaged? etc.). Barrier and enabler analyses can be supported by participatory methods such as community mapping and focus group discussions (Thomas, 2010). Practitioners are then able to identify the critical bottlenecks to be addressed, e.g. physical, attitudes, or institutional etc.(see table below). The Capability, Opportunity, Motivation, Behaviour (COM-B) Model is one methodology that is available and highlights the barriers for each area. The COM-B Model provides sample questions the practitioner should ask in identifying barriers for each area (Government Communication Service, 2021). The “Doer/Non-Doer” practical analysis framework developed by Bonnie (2013) focuses the enablers which have supported the early-adopters the desired behaviour change.
|
Type of barrier |
Barriers |
Solutions |
|
Physical |
• Do not have a latrine and go to the toilet in the bush in the morning • Lack of privacy, fear of insects, feeling ashamed and loss of dignity from defecating in the open • Latrines with high steps and narrow doors. • Unsafe latrine (e.g. no doors or roofs) and dark inside • Crawl or jump into the latrine and get flthy doing this • Wells and pond with no ramps and nothing to hold onto • Paths that are rough and bumpy make it diffcult to get to a water point • Lack of equipment to get water out of the water source and back to the home such as cart, basket, motorized pump |
• Increase accessibility of facilities • Widen doors with level entrances and ramps and handrails instead of steps • Building ramps/rails and widen the path to the water pump |
|
Attitude |
• Isolation in the family/community • High level of discrimination from the community, especially against poor people with disabilities • Limited social support - people with disabilities are not prioritized • Neighbor does not allow people with disability to share the latrine |
• Conduct awareness raising on disability rights – targeting family, community and local authorities (e.g. Commune Councils), to change attitudes towards people with disability Institution/ organisations on water supply and sanitation |
|
Institution/ organisations |
• Lack of information on hygiene for people with disabilities • Lack of plans on WASH for people with disabilities in Commune Investment Plan (CIP) • Limited awareness of existing manuals and guidance • Community and local authorities do not understand about disability rights |
• Conduct hygiene campaigns in different formats to reach people with different impairments • Ensure disability is integrated into various national plans. • Promote plans for WASH for people with disability in local planning process • Promote awareness of approaches to inclusive WASH. • Conduct awareness raising on disability rights – targeting family, community and local authorities (e.g. Commune Councils), to change attitudes towards people with disability |
Table 1. Example of Conducting a Barrier Analysis for WASH Services Accessibility in Pusrat Province, Cambodia (WaterAid, 2015)
2. Developing and Building BCC Materials and Campaign: This is the stage where the designers of the BCC programme decide the message and the communication channel for engagement and interaction with the specific target groups. The messages need to be adapted to the target audience, to their level of knowledge, their challenges, and their perceptions about what can and cannot be done. The messages should be concise, easy to understand, and delivered in a manner that directly applies to them and their behaviour. The F-Diagram is one of the most commonly used BCC materials used in the WASH sub-sector (Figure 2). It is a graphic illustration that describes the potential faecal oral communications pathways which is intended to encourage people to adopt the safe sanitation and hand washing behaviours.
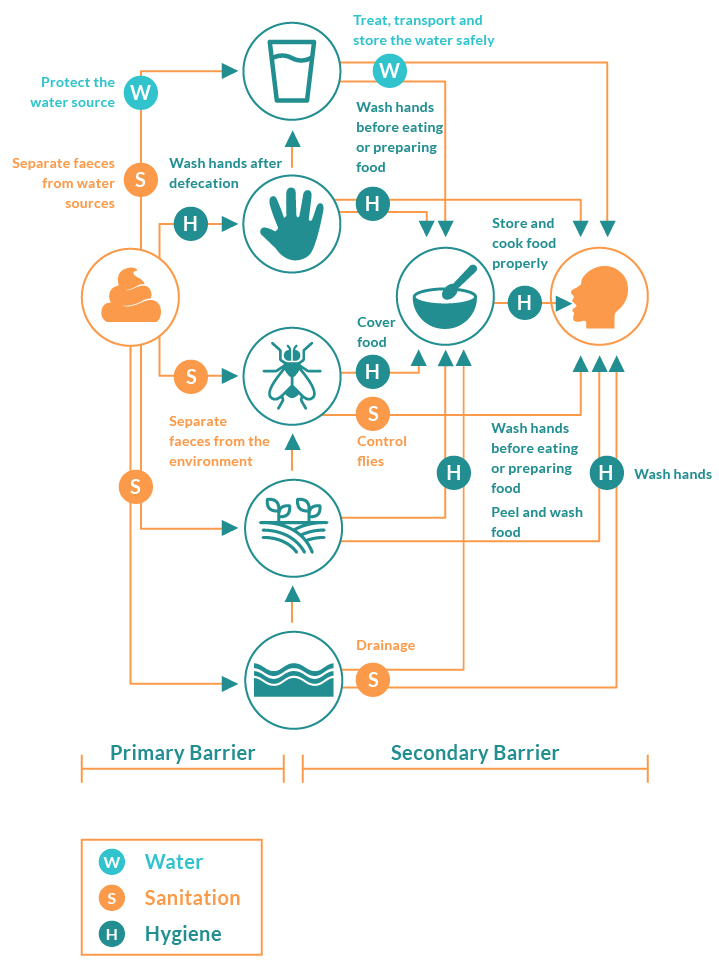
Figure 2. F-Diagram (Adapted from WEDC, 2013)
3. Pretesting: Once the BCC materials and the messages are prepared, pre-testing should be done for its effectiveness and motivation for change. To do so, conduct design workshops or focus groups involving key stakeholders, field workers, and members of the intended audience to also determine the best outlet for dissemination (i.e., print, radio, social media etc.) Then conduct a survey to determine if the produced materials meet the objectives of the programme, the needs of the audience, the message is clear and easy to remember and socially and culturally appropriate (SNV, 2016).
4. Implementation and Messaging: Implementation involves the distribution of created and tested content and messages, implementing the activities that reflect the new behaviour change (e.g., not dumping waste in rivers, hand washing with water and soap after defecations, using household water treatment) and training and capacity building of key players with the necessary skills for creating a multiplier effect for the desired behaviour change. Practical exercises and serious games can help carry out the messaging in a fun, interactive, and effective manner. Great examples have been developed for encouraging handwashing with soap (UNICEF, 2013) and safe menstrual hygiene management (WSSCC, 2016).
5. Monitoring and Evaluation: Refers to the tracking of existing statistics related to the targeted behaviour, tracking outputs to ensure that materials are utilised as planned with desired effects, and tracking the reaction of the target audience to ensure that they are motivated by the materials to change their behaviour (e.g., levels of pollution in rivers over time, % of people reporting washing their hands with water and soap after defecations, and % of households with residual chlorine in their drinking water). Evaluation of the monitoring results will also help identify the lessons learned, where the programme is weak and needs revision, and where it is strong and should be replicated. Feedback from the target groups and stakeholders are absolute necessities as based on these feedbacks, new sets of knowledge can be incorporated into the participant’s lives thus laying the foundation for new sets of behaviour. Additionally, when measuring effectiveness, BCC specialists must make a distinction between three levels; change in behaviour, the communication objective, and the outreach objective (Figure 3).
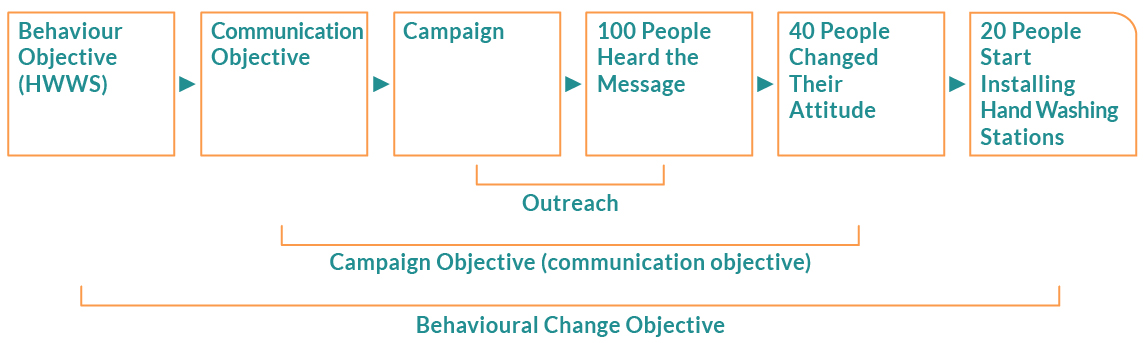
Figure 3. Areas for Consideration when Assessing Effectiveness (Adapted from SNV, 2016)
A successful BCC programme campaign requires extensive participation of the target population and stakeholders in all its stages of development and implementation, especially in the designing stage. The support of the government, health agencies, law enforcement, community leaders and active participation of the target participants is key to running a successful BCC campaign. This support is especially vital for the promotion and sustenance of new behaviour as an individual gradually contemplates, prepares, acts and maintains the newly acquired behaviour. This gradual change is not fixed as the individuals may relapse at any stage, thus calling for constant support. An individual needs a supportive environment for maintaining and sustaining positive changes. This can be done by reducing environmental conditions that support negative behaviours and increasing the conditions that support positive or desired results. Finally, behaviour change studies and programmes cannot be done at the surface level and therefore need to be well resourced (SHARE, 2018).

